
The Storm Before the Storm: An Executive Order, Religious Exemptions, and More
Welcome to our biweekly series in partnership with CIDRAP at the University of Minnesota.
Minneapolis was hit with severe thunderstorms a couple nights ago, so I (Izzy) spent a good chunk of the evening with my dog, swaddled in a blanket, trying to convince her the world wasn’t ending while her teeth chattered through every house-shaking rumble. She knew the storm was coming before I did. She just couldn’t see it on the radar.
I’m still running on very little sleep, and it stuck with me this morning that she sensed the storm before any of us could see it on the radar. That’s not a bad description of how a lot of us are feeling about vaccine policy right now. And I don’t think the unease is unfounded.
Policies and procedures we never could have dreamed could be overturned seem to compound and complicate every time we sit down to write these updates. The American Academy of Pediatrics (AAP) v Kennedy litigation is quiet for now, and most state legislatures have wrapped up—and yet we still don’t feel calm. It is this exact “calm before the storm” window where the administration continues to thrive.
Consider this issue our attempt to show you what’s on that radar as well as we can. But, as with any weather report, it’s subject to change without warning. Let’s discuss…
The PDF version of today’s update is here. Read past installments here and today’s update on the Unbiased Science Substack here.
A Head-Scratching Executive Order
Publicly, the AAP v Kennedy litigation has settled into a waiting game, though there’s plenty happening behind the scenes. Briefing schedules are set and the next hearing isn’t until August. But the administration continues to pursue other options.
We’ve previously covered the back-to-back Advisory Committee on Immunization Practices (ACIP) charter revisions (two in just over a month!) and the pattern this suggests. The second charter, signed by Department of Health and Human Services (HHS) Secretary Robert F. Kennedy Jr. on May 19th, removed some of the language from April’s version while keeping other language broad enough to ensure he retains full authority over the committee’s membership and meeting schedules.
Ten days later, on May 29th, President Donald Trump signed an executive order (EO) directing the Centers for Disease Control and Prevention (CDC) and ACIP to treat the December 2025 HHS scientific assessment as a “guiding resource” and to take steps necessary to realign the childhood vaccine schedule with what it calls “best practices from peer-developed countries.” Jess covered this in depth in her CIDRAP op-ed last week, so we won’t rehash it here, but here’s the short version: the “peer-developed countries” framing is not a valid comparative framework for vaccine policy.

The sequencing of these events is hard to ignore: a newly flexible charter lays the groundwork for new committee appointments followed by an EO that essentially provides marching orders for that committee. Technically speaking, neither move violates Judge Brian Murphy’s March 16th stay, but they were dramatic enough that AAP’s legal team will keep a close watch to ensure they are prepared to respond to any actions that track the same path as before.
Maternal Vaccine Guidelines
This week, the American College of Obstetricians and Gynecologists (ACOG) published its own vaccine schedule for pregnancy, endorsed by 13 medical societies and health organizations. ACOG, as you may remember, is the same organization that withdrew from the ACIP liaison roster in February.
The schedule recommends four vaccines be routinely administered during pregnancy: tetanus, diphtheria, and acellular pertussis (Tdap), respiratory syncytial virus (RSV), influenza, and COVID-19. Additional vaccines are recommended for higher-risk individuals or those who previously missed vaccines.

The CDC’s recommendations for flu and COVID-19 vaccines during pregnancy were withdrawn under Kennedy in December 2025, which means ACOG now directly diverges from the CDC. As Laura Riley of Weill Cornell Medicine noted, vaccination during pregnancy doesn’t just protect the mother, but also newborns who cannot yet be vaccinated. Removing vaccine recommendations from federal guidelines doesn’t erase the biology.
Two years ago, we could have never expected that a major professional society would have to correct rampant vaccine misinformation coming from federal guidance. Today, it’s sadly routine.
What ‘Decoupling from the CDC’ Actually Means
This was the top comment we received from last issue’s survey, so here’s our plain-language explainer.
Over the past several decades, most U.S. vaccine policy has operated as though it’s a well-oiled machine. The ACIP reviewed evidence and issued recommendations. Under the Affordable Care Act, insurance coverage was tied to those recommendations, which meant any vaccine on the recommended schedule had to be covered. The CDC schedule served as the universal foundation from which states could build, adding their own school-entry requirements.
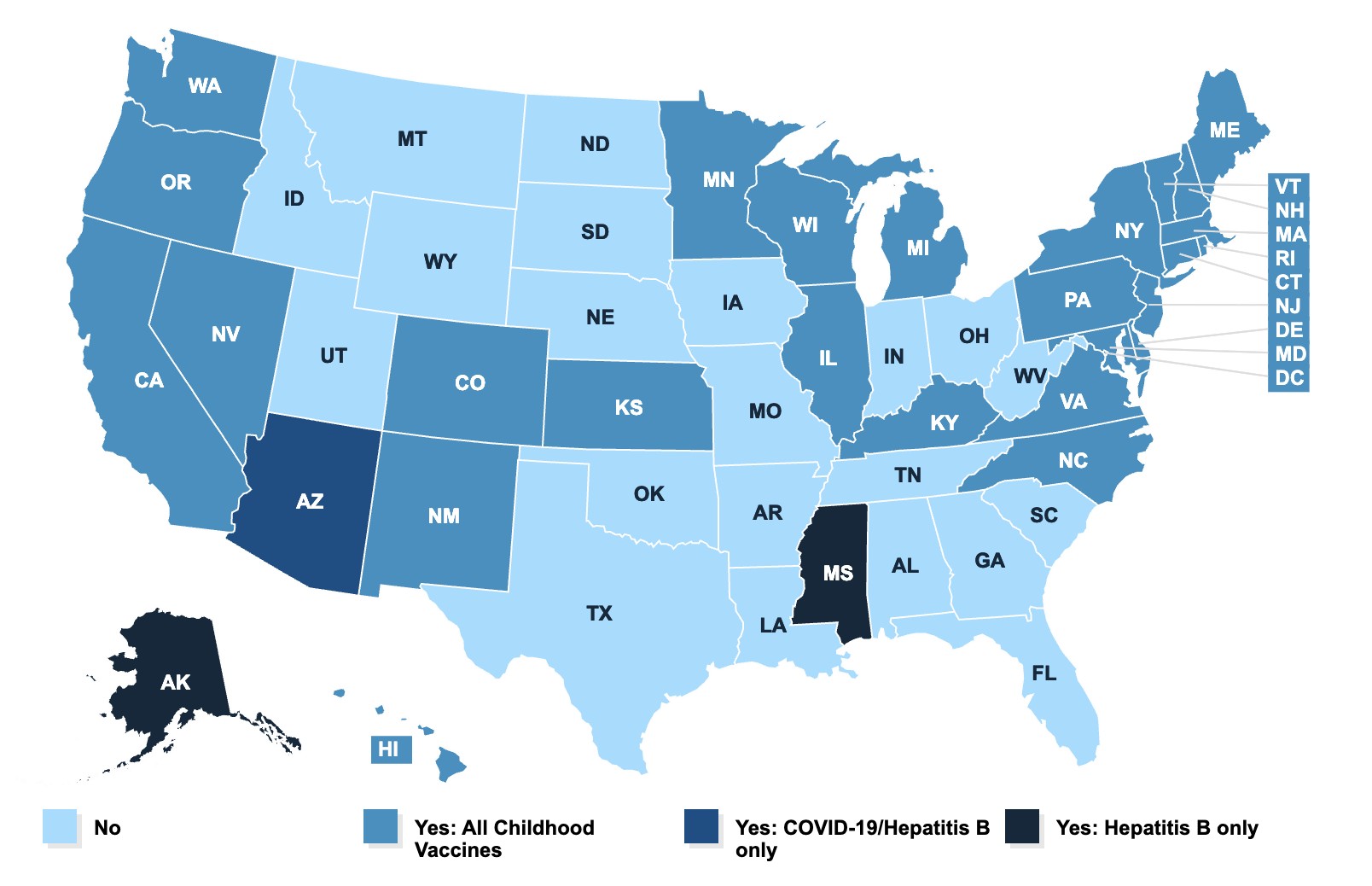
You’ve already seen what it looks like when that machine starts to rust. At the professional society level, ACOG is issuing its own guidance, because it no longer trusts the federal body to act in a pregnant woman’s best interest. As we’ve covered in our state roundups, at least a dozen states are now tying their recommendations to organizations like the AAP, or their own state health officer’s judgment, rather than the federal schedule. And finally, at the federal level, the ACIP is in legal limbo, and in any practical sense there is no functional recommending body at this time.
The way that decoupling acts in practice is, for lack of a better term, chaos. A pregnant woman in Maryland seeing an OB-GYN affiliated with a major academic medical center will likely receive flu and COVID-19 vaccine recommendations this fall. A pregnant woman in Texas, where there is no decoupling legislation, who sees a provider that only follows CDC guidance may not. A teenager in Iowa who wants to receive the HPV vaccine now needs parental consent to receive it. Meanwhile, a child in Maine can receive it at a pharmacy without a prescription.
Decoupling recommendations from the CDC is currently the best option for operating within a system that previously has never seen such fragmentation. The patchwork system that we now find ourselves operating in maps closely onto political geography, so it’s not random, per se. And while this is seemingly the best option for now, the complexity is affecting real clinical decisions and disease risk differentially across different demographic groups nationwide.
State Round-Up
The wave of vaccine-related bills we’ve been tracking has slowed considerably. Louisiana SB 29 was signed into law on June 2 (now Act 732, effective August 1), requiring coroners to include a child’s immunization history in autopsy reports for sudden child deaths, a framing that implies a vaccine link that the evidence doesn’t support.
In Arizona, HB 2248, the “Arizona Medical Freedom Act,” heads to the governor’s desk; it would bar schools, businesses, employers, and government from requiring “medical interventions,” a term defined broadly enough to cover vaccines. Coupled with Arizona’s HB 2048, which is also advancing to the governor’s desk, this could remove school vaccine requirements entirely. And Illinois adopted two symbolic resolutions, HR 810 and HR 803, declaring Vaccine Awareness Day and Hepatitis B Awareness Day.
On Religious Exemptions
While the legislative push to weaken vaccines has had mixed outcomes in state houses this session, the legal strategy is a different story. According to a Washington Post analysis published this week, the next page in the so-called “anti-vaccine movement” playbook to ensure a national win through the courts will likely operate through claims on First Amendment religious freedoms.
The central case in question is Miller v. McDonald(filed in 2023), in which Amish parents are challenging the state of New York’s refusal to recognize religious vaccine exemptions. The Supreme Court sent the case back to the 2nd Circuit in December, and if the 2nd Circuit still rejects a religious exemption, the case would likely make it back to the Supreme Court. Here, a ruling in the plaintiffs’ favor could essentially require religious exemptions across the country. Cases in West Virginia and California are also advancing. Aaron Siri has been the driving force behind much of this litigation.
Lawrence Gostin of Georgetown University called a potential court win “the worst nightmare for public health,” warning that it could function as a blanket opt-out system for anyone, given current levels of vaccine misinformation and distrust.
Importantly, legislative and legal strategies don’t require the same conditions to succeed. The legislative push started slowly because it was polling as a liability heading into the midterms. Litigation, however, doesn’t answer to voters. These cases will move ahead regardless of November midterm election results, and the Court’s more recent posture on religious liberties suggests that the current legal environment may be the most favorable it’s been to these challenges in decades.
Fall Vaccine Composition: COVID-19 and Flu
The U.S. Food and Drug Administration’s (FDA) Vaccines and Related Biological Products Advisory Committee (VRBPAC) met on May 28th and recommended that the fall 2026-2027 COVID-19 vaccine target the XFG strain. While this differs from the World Health Organization’s (WHO) strain selection of LP.8.1, it’s not unusual for these recommendations to diverge. The WHO’s guidance is intended to cover all member countries, while VRBPAC focuses just on what’s circulating or expected to circulate in the U.S. The FDA will make the final determination.
VRBPAC will meet again on June 18th to make recommendations on Moderna’s new mRNA influenza vaccine for individuals 50 years of age and older.
Aside from the actual vaccine composition, the next steps get a little more complicated. As Katherine J. Wu explains in The Atlantic, after VRBPAC decides on the composition of the vaccines, the ACIP would usually convene to recommend who should receive these vaccines. This guidance directly affects the Vaccines for Children (VFC) program, which covers more than half of American kids.
There’s currently no functioning CDC. Last fall, the delayed COVID-19 vaccine guidance issued by the ACIP caused confusion for pharmacies, clinicians, and those in charge of ordering the vaccines across multiple states. As it stands, experts are warning that a similar situation is very possible this fall.
What Else We’re Watching
- Trust in the CDC is falling, but support for childhood vaccines is holding. A new poll from the de Beaumont Foundation and Harvard T.H. Chan School of Public Health found that only 50% of adults said they could rely on the CDC for health recommendations (down from 77% last year). Yet, more than three-quarters of the public still supports school vaccination requirements.
- RFK Jr. is seeking access to Americans’ medical records to revisit the vaccine-autism question. HHS is pursuing data from state health information exchanges—which let hospitals and clinics share detailed, identifiable patient records—to research a vaccine-autism link the medical establishment has long rejected. Some public health leaders objected in private meetings, doubting it’s legal or useful, and HHS has offered no detail on how it would protect the information. Maryland declined to share data, while a Nebraska nonprofit cooperated as millions in federal dollars flowed to the effort.
- Merck settled the bulk of its Gardasil lawsuits for approximately $50 million. Though it may seem like an admission of liability, it’s not. Settlements are driven by many factors including litigation cost and risk management. The scientific consensus on human papillomavirus (HPV) vaccine safety has not changed.
- The U.S. signaled it will re-engage with Gavi, the Vaccine Alliance. Secretary of State Marco Rubio told the Senate Foreign Relations Committee on June 2 that the U.S. would re-engage with Gavi amid the Ebola outbreak in several African countries. Kennedy had been holding up $600 million that Congress appropriated for fiscal 2025 and 2026, in part because Gavi declined to phase out the preservative thimerosal. The funds expire September 30 if the administration doesn’t release them. The reversal is notable, given that Kennedy framed the original cutoff around vaccine-safety claims he never substantiated.
- The Office of Management and Budget (OMB) proposed a sweeping rework of federal grant oversight. The proposed rule would significantly affect how research is both funded and conducted across the National Institutes of Health and other agencies. Individual comments carry more weight than form letters, and comments don’t need to be long or technical. The public comment period is open until July 13 if you would like to submit something.
This issue has been a bit dreary, but we do have some exciting news to share! We’re launching a dedicated inbox for reader questions about vaccines and vaccine policy. Whether it’s something you’ve seen in the news, a claim a family member shared, or a policy question you can’t find a straight answer to, send it to vaccines@unbiasedscience.com. We can’t promise we’ll answer every question individually, but we will use those questions to shape future newsletter and social media content. We can’t wait to hear from you! (And as always, you’re welcome to leave your comments and questions right here on our Substack, too.)
Stay curious,
Unbiased Science











